

BACKGROUND:
Children with high risk acute myeloid leukemia (AML) still experience consistently high rates of relapse. Survival after first relapse increased from 21% between 1987 and 1997 up to 39% in recent studies. However, since 2009, there have been no publications on subsequent large pediatric AML relapse trials. As the indications for HSCT during first-line treatment have been extended since then, the current survival of these patients at relapse remains unclear.
Herein, we report outcome results from the BFM and COG study group, which represents the largest available dataset analyzed for post-relapse survival.
PATIENTS AND METHODS:
Pediatric patients with first relapse of AML (no Down syndrome, secondary leukemia or FAB M3) have been analyzed from two large study groups with patients from the United States, Canada, Australia, New Zealand, Germany, Austria, Czech Republic and Switzerland. Out of 1222 patients in the BFM cohort (AML-BFM study 2004, registry 2012 and study 2012), 350 experienced at least one relapse and 197 of those had a first relapse after closure of the last I-BFM relapse trial (04/2009 through 2017). Within the Children's Oncology Group (COG) Phase 3 trials (AAML0531 and AAML1031, n=2119) 852 pediatric patients suffered a relapse.
Five-year probability of overall survival (pOS) and event-free survival (pEFS) were calculated according to Kaplan-Meier. EFS was calculated for the BFM cohort as time from relapse to the next event (second relapse, death, failure to achieve a second remission or secondary malignancy) or until last follow-up, while OS reflects the time from relapse until death or last follow-up. The Cox proportional hazards model was used for multivariate analysis of outcomes. Living patients were censored at last follow-up with a median follow-up after relapse of 4·2 years (BFM) and 4·8 years (COG). Data have been frozen at 03/27/2020 (BFM) and 03/31/2020 (COG).
RESULTS:
In the 197 patients with relapse after closure of the last BFM relapse trial (04/2009 through 2017) the pOS at 5 years was 42±4% (BFM). The 5-year pOS in patients relapsing after COG trials 2006-2018 was 35±2% (n=852). Patients experiencing a relapse between 2014 to 2017 had a pOS of 49±6% (BFM, n=78) and 40±3% (COG, n=333).
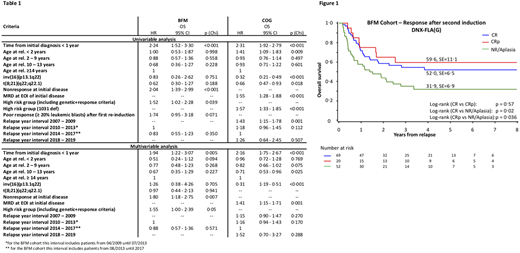
Risk classification at initial diagnosis and a short time from diagnosis to relapse predicted a diminished survival probability in both cohorts (see Table 1). However, the absence of full hematopoietic regeneration of the bone marrow after re-induction did not predict survival: Within the BFM dataset, a subgroup analysis in all patients receiving DNX-FLA (n=156) have been performed. Initial characteristics are comparable to the total cohort. Among these patients 147 were evaluable for response (7 excluded due to early death before evaluation, 2 for insufficient data). Eighty-nine (57%) achieved a CR (n=69) or CRp (n=20) and 52 (33%) no response. Overall survival was superior for patients with a CR/CRp (54±6% (CR/CRp) vs. 32±7% (No CR/CRp); p=0·0064), but long-term survival was still possible even with a poor re-induction response. Patients with a CRp had a comparable survival to those with a CR after a second re-induction (pOS 60±11% (CRp) vs. pOS 52±7% (CR); p=0·57). Patients with >5% leukemic blasts (n=32) had the lowest survival (pOS 27±9%). The 5-year pEFS for this cohort was 29±4% (pEFS 50±6% (CR) vs. pEFS 50±11% (CRp)).
The analysis of post-relapse treatment showed that the vast majority of patients who survive had a HSCT following relapse. By landmark analysis, survival was significantly higher in patients with subsequent HSCT compared to that of non-transplanted patients (BFM: pOS 53±4%, n=154 vs. pOS 5±5%, n=21; p(Mantel-Byar)=0·0002).
CONCLUSION:
This is the largest report to date on post relapse survival in children with AML. Our analysis confirmed previously described risk factors for poor survival while also highlighting new findings contrary to established standards. Strikingly, the absence of full hematopoietic regeneration of the bone marrow after re-induction did not predict survival at first relapse, thereby questioning the current value of the established International Working Group Criteria published by Cheson et al for response-evaluation in pediatric AML. As the international pediatric AML community embarks on collaborative efforts to evaluate new therapies in children with relapsed AML, a comprehensive review of post relapse survival is critical.
Bourquin:Servier: Other: Travel Support. Reinhardt:Novartis: Membership on an entity's Board of Directors or advisory committees; CLS Behring: Research Funding; bluebird bio: Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees; Roche: Research Funding; Celgene Corporation: Membership on an entity's Board of Directors or advisory committees, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal